|
|
|
|
|
|
Review |
Sukhatme et al., Front. Pharmacol., doi:10.3389/fphar.2021.652688 (Review) (Peer Reviewed) |
review |
Fluvoxamine: A Review of Its Mechanism of Action and Its Role in COVID-19 |
|
Details
Review of mechanisms of action of fluvoxamine and other SSRIs that could be beneficial for COVID-19 treatment, including lower platelet aggregation, decreased mast cell degranulation, interference with endolysosomal viral trafficking, reg.. |
|
Details
Source
PDF
Review
Review
|
| Sukhatme et al., Front. Pharmacol., doi:10.3389/fphar.2021.652688 (Review) (Peer Reviewed) |
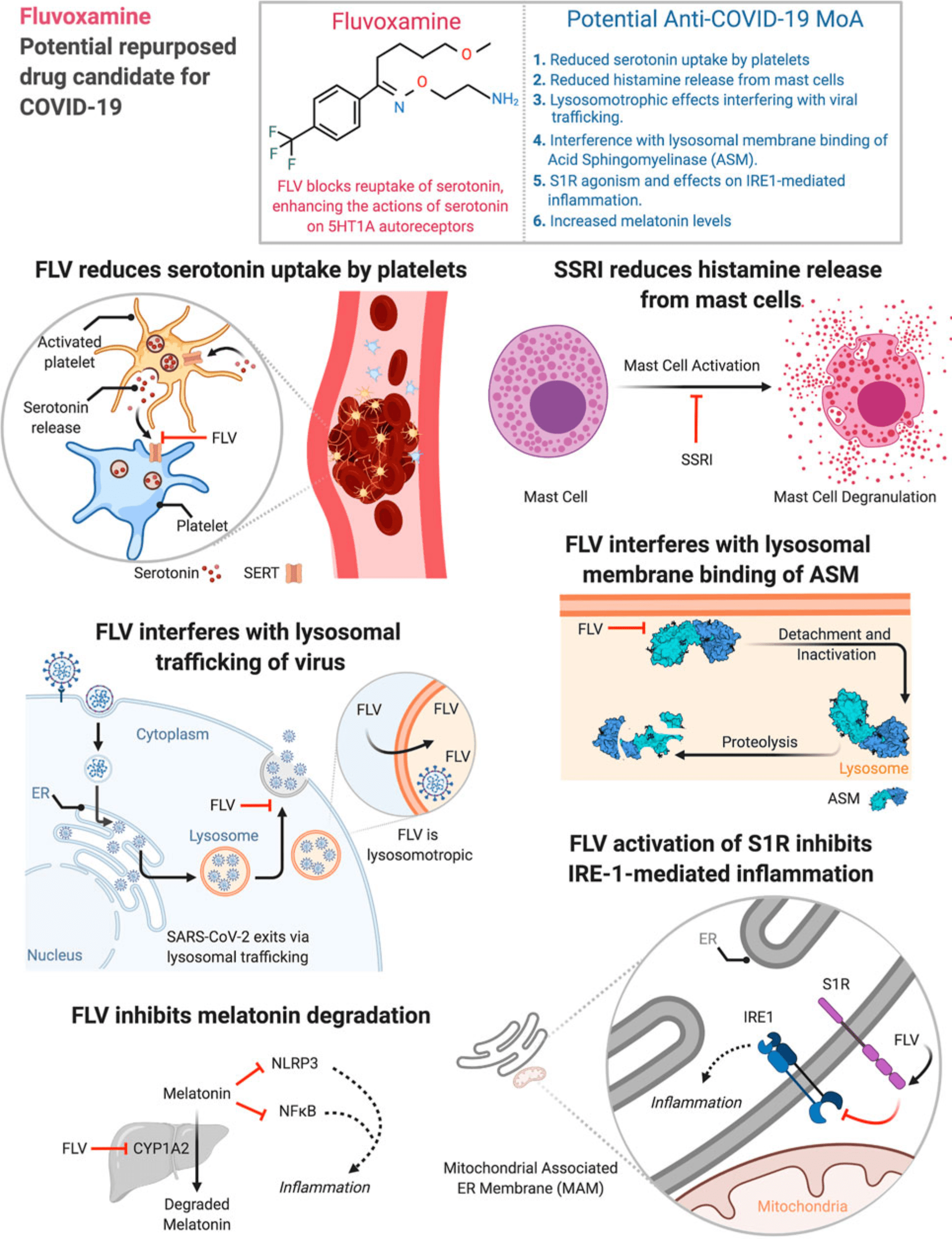
| Fluvoxamine: A Review of Its Mechanism of Action and Its Role in COVID-19 |
Review of mechanisms of action of fluvoxamine and other SSRIs that could be beneficial for COVID-19 treatment, including lower platelet aggregation, decreased mast cell degranulation, interference with endolysosomal viral trafficking, regulation of inositol-requiring enzyme 1α-driven inflammation, and increased melatonin levels.
![]()
Sukhatme et al., 4/20/2021, peer-reviewed, 4 authors.
|
|
Submit Corrections or Comments
|
|
Review |
Kirsch, S. (Review) (Preprint) |
review |
COVID FAQ |
|
Details
COVID FAQ from the founder of the COVID-19 Early Treatment Fund [1], including an extensive analysis of the fluvoxamine trials and other supporting evidence. |
|
Details
Source
PDF
Review
Review
|
| Kirsch, S. (Review) (Preprint) |
| COVID FAQ |
|
COVID FAQ from the founder of the COVID-19 Early Treatment Fund [1], including an extensive analysis of the fluvoxamine trials and other supporting evidence.
Kirsch et al., 3/6/2021, preprint, 1 author.
|
|
Submit Corrections or Comments
|
|
Early |
Seftel et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofab050 (Peer Reviewed) |
death/ICU, ↓83.9%, p=0.15 |
Prospective cohort of fluvoxamine for early treatment of COVID-19 |
|
Details
Prospective quasi-randomized (patient choice) study with 125 outpatients, 77 treated with fluvoxamine, showing lower death/ICU admission (0 of 77 vs. 2 of 48), lower hospitalization (0 of 77 vs. 6 of 48), and faster recovery with treatmen.. |
|
Details
Source
PDF
Early treatment study
Early treatment study
|
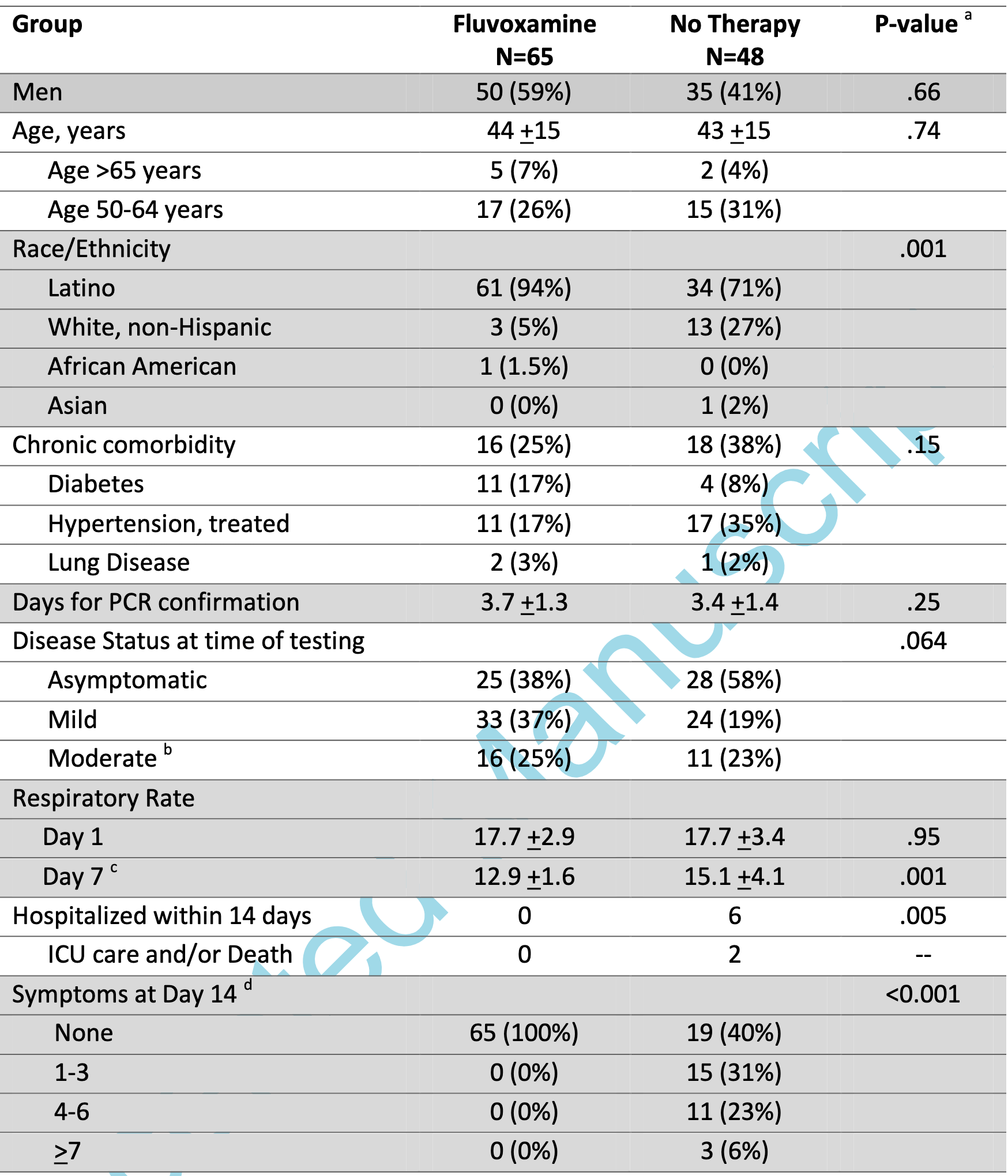
| Seftel et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofab050 (Peer Reviewed) |
| Prospective cohort of fluvoxamine for early treatment of COVID-19 |
Prospective quasi-randomized (patient choice) study with 125 outpatients, 77 treated with fluvoxamine, showing lower death/ICU admission (0 of 77 vs. 2 of 48), lower hospitalization (0 of 77 vs. 6 of 48), and faster recovery with treatment. Note that 12 treatment patients were added but are not reflected in the table in the paper (because the numbers had been previously published and the IRB did not allow updating the table).
![]()
risk of combined death/ICU, 83.9% lower, RR 0.16, p = 0.15, treatment 0 of 77 (0.0%), control 2 of 48 (4.2%), continuity correction due to zero event.
risk of hospitalization, 94.0% lower, RR 0.06, p = 0.003, treatment 0 of 77 (0.0%), control 6 of 48 (12.5%), continuity correction due to zero event.
risk of no recovery, 98.7% lower, RR 0.01, p < 0.001, treatment 0 of 77 (0.0%), control 29 of 48 (60.4%), continuity correction due to zero event.
Seftel et al., 2/1/2021, prospective quasi-randomized (patient choice), USA, North America, peer-reviewed, 2 authors.
|
|
Submit Corrections or Comments
|
|
Early |
Lenze et al., JAMA, doi:10.1001/jama.2020.22760 (Peer Reviewed) |
progression, ↓92.7%, p=0.009 |
Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial |
|
Details
RCT 152 outpatients, 80 treated with fluvoxamine showing lower progression with treatment (0 of 80 versus 6 of 72 control). |
|
Details
Source
PDF
Early treatment study
Early treatment study
|
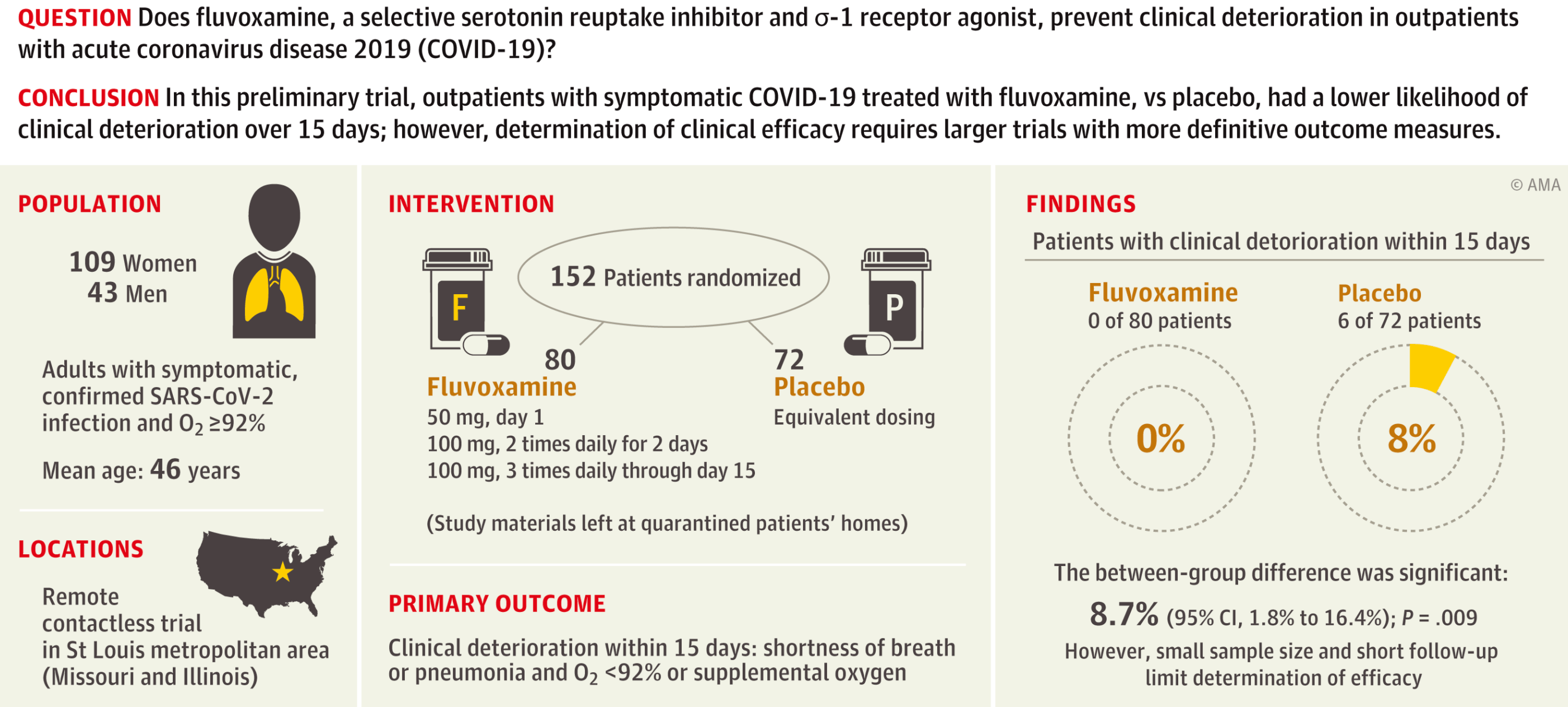
| Lenze et al., JAMA, doi:10.1001/jama.2020.22760 (Peer Reviewed) |
| Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial |
RCT 152 outpatients, 80 treated with fluvoxamine showing lower progression with treatment (0 of 80 versus 6 of 72 control).
![]()
risk of disease progression, 92.7% lower, RR 0.07, p = 0.009, treatment 0 of 80 (0.0%), control 6 of 72 (8.3%), continuity correction due to zero event, clinical deterioration over 15 days.
risk of hospitalization, 82.0% lower, RR 0.18, p = 0.009, treatment 1 of 80 (1.2%), control 5 of 72 (6.9%), COVID-19 hospitalization within 15 days, see supplemental appendix for details.
Lenze et al., 11/12/2020, Double Blind Randomized Controlled Trial, peer-reviewed, 11 authors.
|
|
Submit Corrections or Comments
|
|
Late |
Hoertel et al., Molecular Psychiatry, doi:10.1038/s41380-021-01021-4 (Peer Reviewed) |
Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: results from an observational study |
|
Details
Retrospective 7,230 hospitalized COVID-19 patients in France, 345 receiving an antidepressant medication within 48 hours of admission. There was a significant association between antidepressant use and reduced risk of intubation or death .. |
|
Details
Source
PDF
Late treatment study
Late treatment study
|
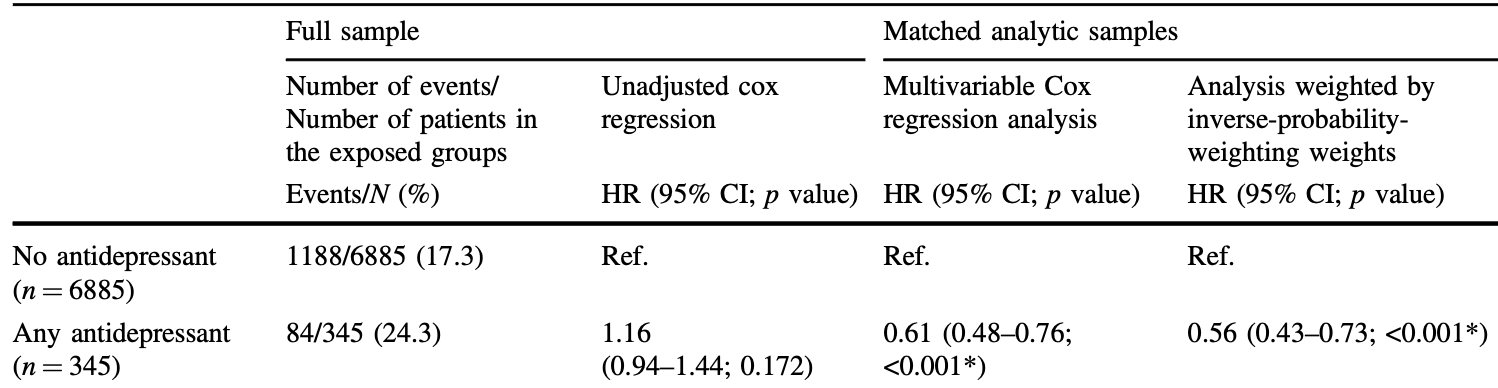
| Hoertel et al., Molecular Psychiatry, doi:10.1038/s41380-021-01021-4 (Peer Reviewed) |
| Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: results from an observational study |
Retrospective 7,230 hospitalized COVID-19 patients in France, 345 receiving an antidepressant medication within 48 hours of admission. There was a significant association between antidepressant use and reduced risk of intubation or death (HR 0.56, p < 0.001). Fluvoxamine is not included because there was only one person taking it in this study.
![]()
Hoertel et al., 8/17/2020, peer-reviewed, 17 authors.
|
|
Submit Corrections or Comments
|
Please send us corrections, updates, or comments. Vaccines and treatments are both extremely valuable and complementary. All
practical, effective, and safe means should be used. Elimination of COVID-19
is a race against viral evolution. No treatment, vaccine, or intervention is
100% available and effective for all current and future variants. Denying the
efficacy of any method increases the risk of COVID-19 becoming endemic; and
increases mortality, morbidity, and collateral damage. We do not provide
medical advice. Before taking any medication, consult a qualified physician
who can provide personalized advice and details of risks and benefits based
on your medical history and situation. Treatment protocols for physicians are
available from the FLCCC.
Thanks for your feedback! Please search before submitting papers and note
that studies are listed under the date they were first available, which may be
the date of an earlier preprint.
Submit
{kind=link}
{kind=link}
{kind=link}
{kind=link}