1 February 2021 - Early treatment study
Prospective cohort of fluvoxamine for early treatment of COVID-19
et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofab050 (Peer Reviewed)
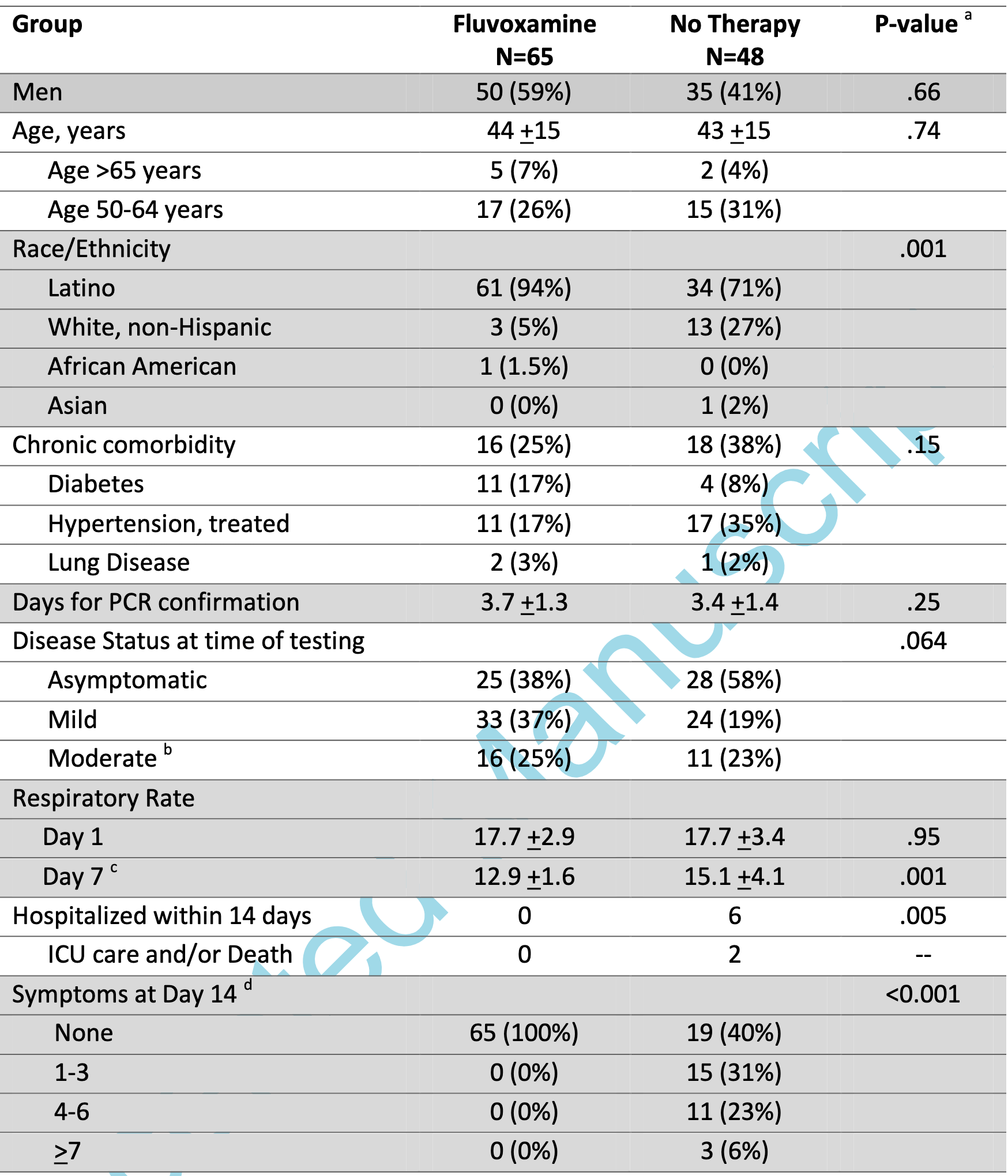
Prospective quasi-randomized (patient choice) study with 125 outpatients, 77 treated with fluvoxamine, showing lower death/ICU admission (0 of 77 vs. 2 of 48), lower hospitalization (0 of 77 vs. 6 of 48), and faster recovery with treatment. Note that 12 treatment patients were added but are not reflected in the table in the paper (because the numbers had been previously published and the IRB did not allow updating the table).
|
risk of death/ICU, 83.9% lower, RR 0.16, p = 0.15, treatment 0 of 77 (0.0%), control 2 of 48 (4.2%), NNT 24, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm).
|
|
risk of hospitalization, 94.0% lower, RR 0.06, p = 0.003, treatment 0 of 77 (0.0%), control 6 of 48 (12.5%), NNT 8.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm).
|
|
risk of no recovery, 98.7% lower, RR 0.01, p < 0.001, treatment 0 of 77 (0.0%), control 29 of 48 (60.4%), NNT 1.7, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm).
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. |
Seftel et al., 2/1/2021, prospective quasi-randomized (patient choice), USA, North America, peer-reviewed, 2 authors.
Please send us
corrections, updates, or comments. Vaccines and treatments are both
valuable and complementary. All practical, effective, and safe means
should be used. Elimination of COVID-19 is a race against viral evolution. No
treatment, vaccine, or intervention is 100% available and effective for all
current and future variants. Denying the efficacy of any method increases
mortality, morbidity, collateral damage, and the risk of endemic status. We do
not provide medical advice. Before taking any medication, consult a qualified
physician who can provide personalized advice and details of risks and
benefits based on your medical history and situation. WCH
and FLCCC provide
treatment protocols.