

Covid Analysis, January 2, 2022, DRAFT
https://c19fluvoxamine.com/meta.html
•Statistically significant improvements are seen for mortality and recovery. 4 studies from 4 independent teams in 3 different countries show statistically significant
improvements in isolation (1 for the most serious outcome).
•Meta analysis using the most serious outcome reported shows
34% [7‑53%] improvement. Results are similar for Randomized Controlled Trials and similar for peer-reviewed studies. Early treatment is more effective than late treatment.
•While many treatments have some level
of efficacy, they do not replace vaccines and other measures to avoid
infection.
Only 33% of fluvoxamine
studies show zero events in the treatment arm.
•Multiple treatments are typically used
in combination, and other treatments
may be more effective.
•Elimination of COVID-19 is a race
against viral evolution. No treatment, vaccine, or intervention is 100%
available and effective for all variants. All practical, effective, and safe
means should be used, including treatments, as supported by Pfizer [Pfizer].
Denying the efficacy of treatments increases the risk of COVID-19 becoming
endemic; and increases mortality, morbidity, and collateral damage.
•All data to reproduce this paper and
sources are in the appendix.
| Studies | Early treatment | Late treatment | Prophylaxis | Patients | Authors | |
| All studies | 6 | 64% [-93‑93%] | 40% [23‑53%] | -58% [-493‑58%] | 2,599 | 56 |
| Peer-reviewed | 5 | 89% [15‑99%] | 40% [23‑53%] | -58% [-493‑58%] | 2,052 | 55 |
| Randomized Controlled TrialsRCTs | 3 | 62% [-310‑96%] | 30% [-26‑63%] | 2,196 | 39 | |
| Percentage improvement with fluvoxamine treatment | ||||||
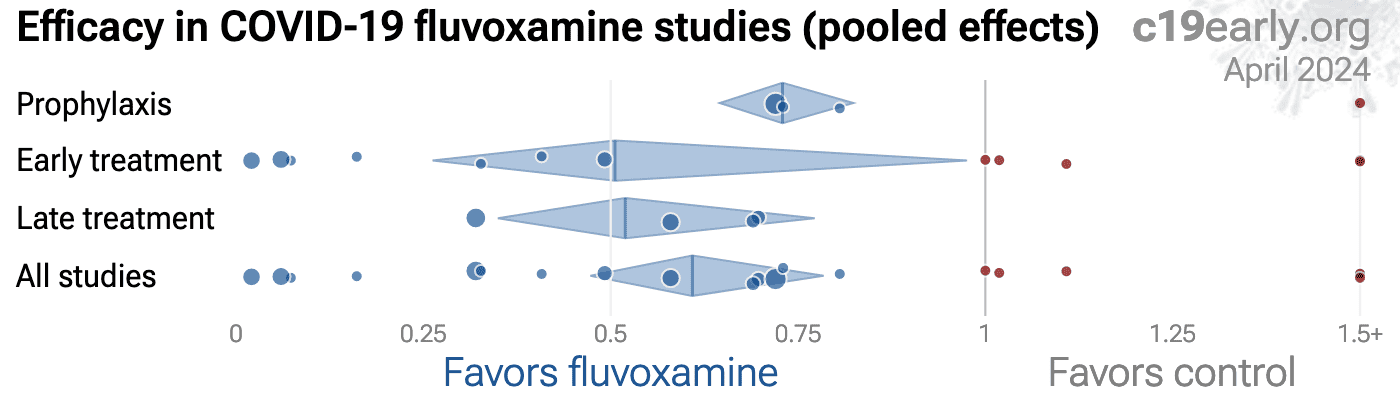

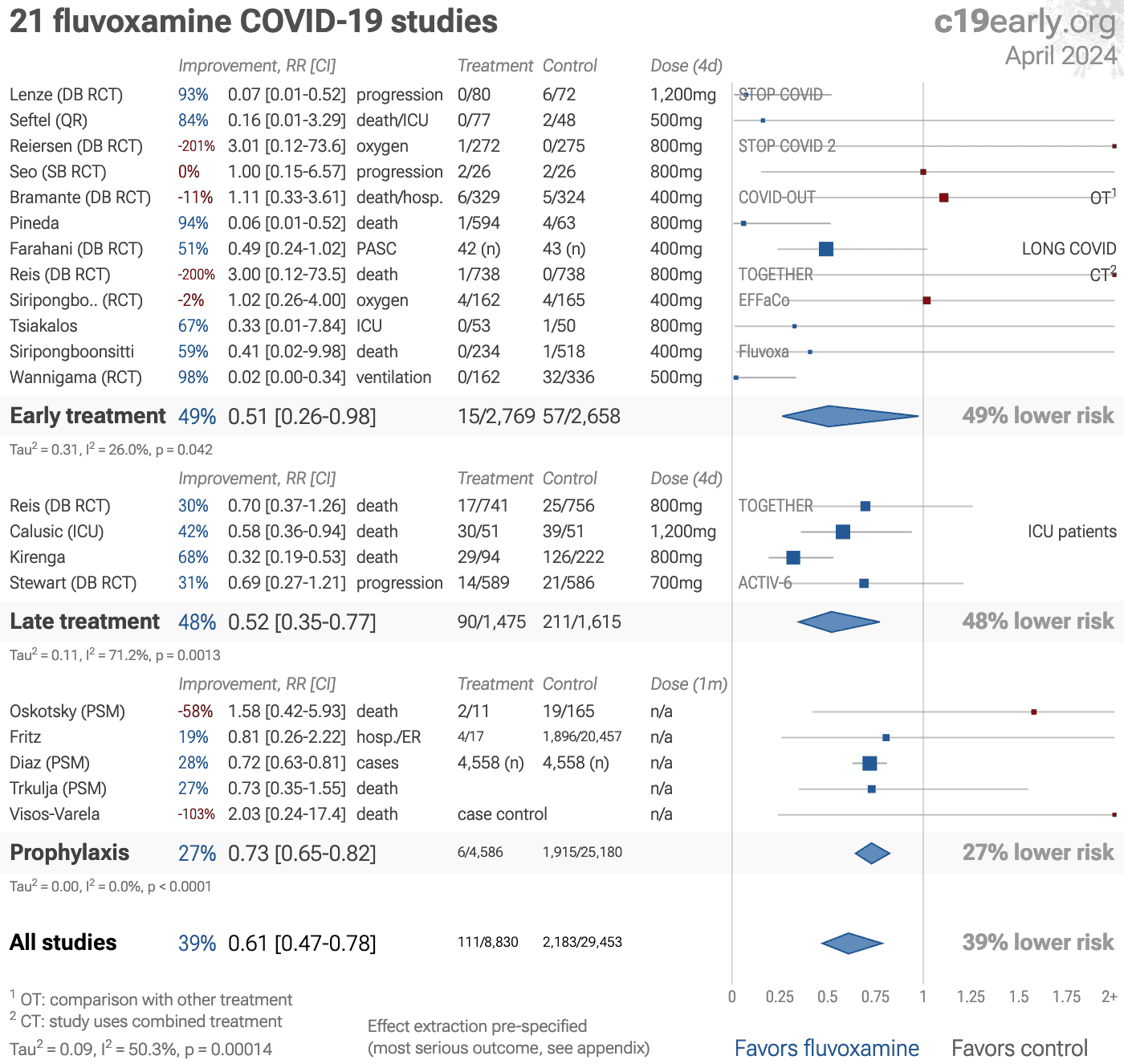
Figure 1. A. Random effects
meta-analysis. This plot shows pooled effects, discussion can be found in the heterogeneity section,
and results for specific outcomes can be found in the individual outcome analyses.
Effect extraction is pre-specified, using the most serious outcome reported.
For details of effect extraction see the appendix.
B. Scatter plot showing the
distribution of effects reported in studies. C. History of all reported
effects (chronological within treatment stages).
Introduction
We analyze all significant studies concerning the use of
fluvoxamine for COVID-19. Search methods, inclusion criteria, effect
extraction criteria (more serious outcomes have priority), all individual
study data, PRISMA answers, and statistical methods are detailed in
Appendix 1. We present random effects meta-analysis results for all
studies, for studies within each treatment stage, for individual outcomes, for
peer-reviewed studies, for Randomized Controlled Trials (RCTs), and after
exclusions.
Figure 2 shows stages of possible treatment for
COVID-19. Prophylaxis refers to regularly taking medication before
becoming sick, in order to prevent or minimize infection. Early
Treatment refers to treatment immediately or soon after symptoms appear,
while Late Treatment refers to more delayed treatment.
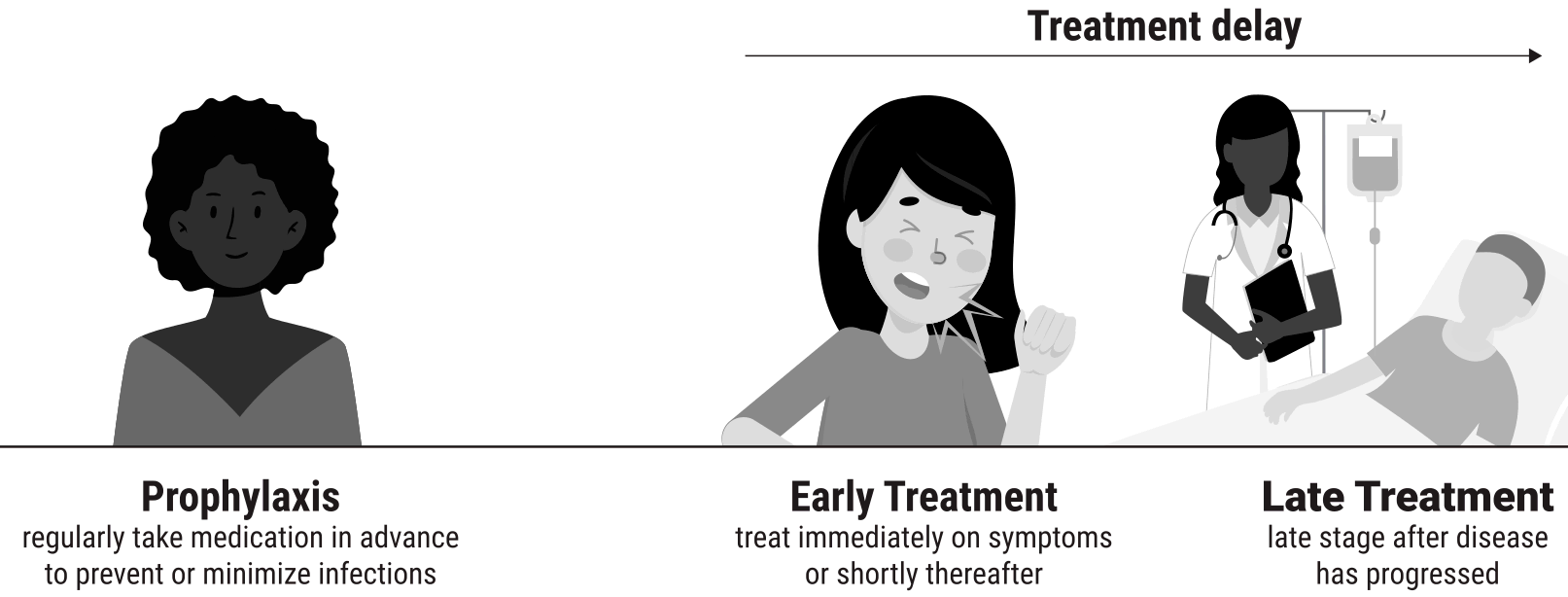
Figure 2. Treatment stages.
Mechanisms of Action
| FIASMA | Fluvoxamine is a functional inhibitor of acid sphingomyelinase (FIASMA). SARS-CoV-2 activates the ASM/ceramide system which may facilitate viral entry. ASM inhibition may reduce the concentration of ceramides and inhibit viral entry [Carpinteiro, Carpinteiro (B), Hoertel]. |
| Sigma-1 activation | Fluvoxamine may reduce clinical deterioration via σ-1 (S1R) receptor activation, which regulates cytokine production [Hashimoto, Sukhatme]. |
| Platelet activation | Platelet activation may contribute to COVID-19 severity. Fluvoxamine inhibits platelet activation [Battinelli, Sukhatme]. |
| Lysosomal trafficking | SARS-CoV-2 uses lysosomal trafficking to escape from infected cells. Fluvoxamine is lysosomotropic and interferes with endolysosomal viral trafficking [Norinder, Sukhatme]. |
| Heme oxygenase | COVID-19 risk may be related to low intracellular heme oxygenase (HO-1). Fluvoxamine increases HO-1 and HO-1 has cytoprotective and anti-inflammatory properties [Almási, Hooper, Hooper (B)]. |
| Mast cell degranulation | Fluvoxamine may reduce cytokine storm due to decreased mast cell degranulation [Sukhatme]. |
| Melatonin | Melatonin may be beneficial for COVID-19, and fluvoxamine may elevate melatonin levels via CYP1A2 and CYP2C19 inhibition [Anderson, Camp, Ramos, Sukhatme]. |
Table 1. Fluvoxamine mechanisms of action.
Submit updates.
Results
Figure 3, 4, 5, 6, 7, 8, 9, and 10
show forest plots for a random effects meta-analysis of
all studies with pooled effects, mortality results, ventilation, hospitalization, progression, recovery, viral clearance, and peer reviewed studies.
Table 2 summarizes the results by treatment stage.
| Treatment time | Number of studies reporting positive effects | Total number of studies | Percentage of studies reporting positive effects | Random effects meta-analysis results |
| Early treatment | 3 | 3 | 100% |
64% improvement RR 0.36 [0.07‑1.93] p = 0.24 |
| Late treatment | 2 | 2 | 100% |
40% improvement RR 0.60 [0.47‑0.77] p < 0.0001 |
| Prophylaxis | 0 | 1 | 0.0% |
-58% improvement RR 1.58 [0.42‑5.93] p = 0.51 |
| All studies | 5 | 6 | 83.3% |
34% improvement RR 0.66 [0.47‑0.93] p = 0.017 |
Table 2. Results by treatment stage.
Figure 3. Random effects meta-analysis for all studies with pooled effects.
This plot shows pooled effects, discussion can be found in the heterogeneity section,
and results for specific outcomes can be found in the individual outcome analyses.
Effect extraction is pre-specified, using the most serious outcome reported.
For details of effect extraction see the appendix.
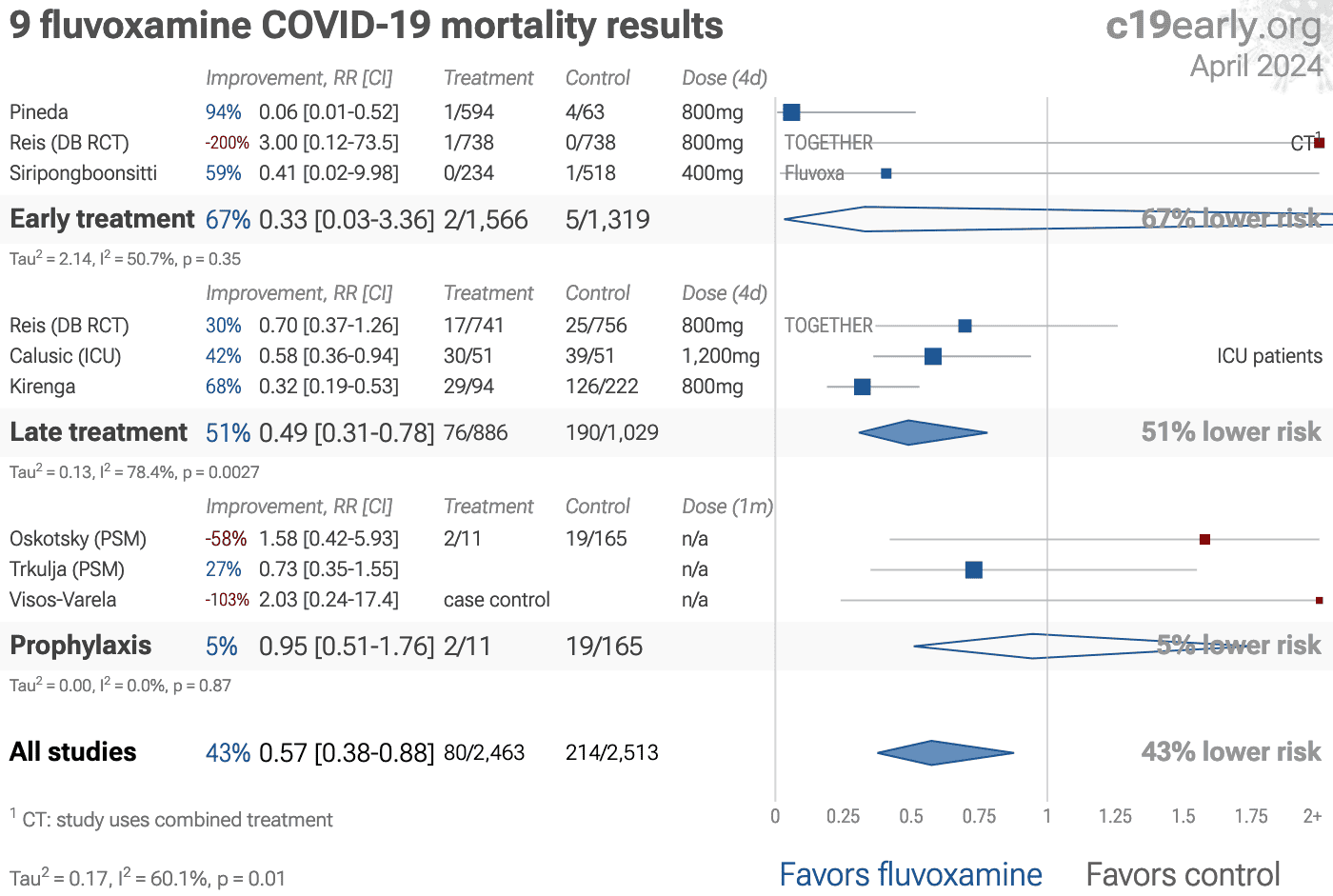
Figure 4. Random effects meta-analysis for mortality results.
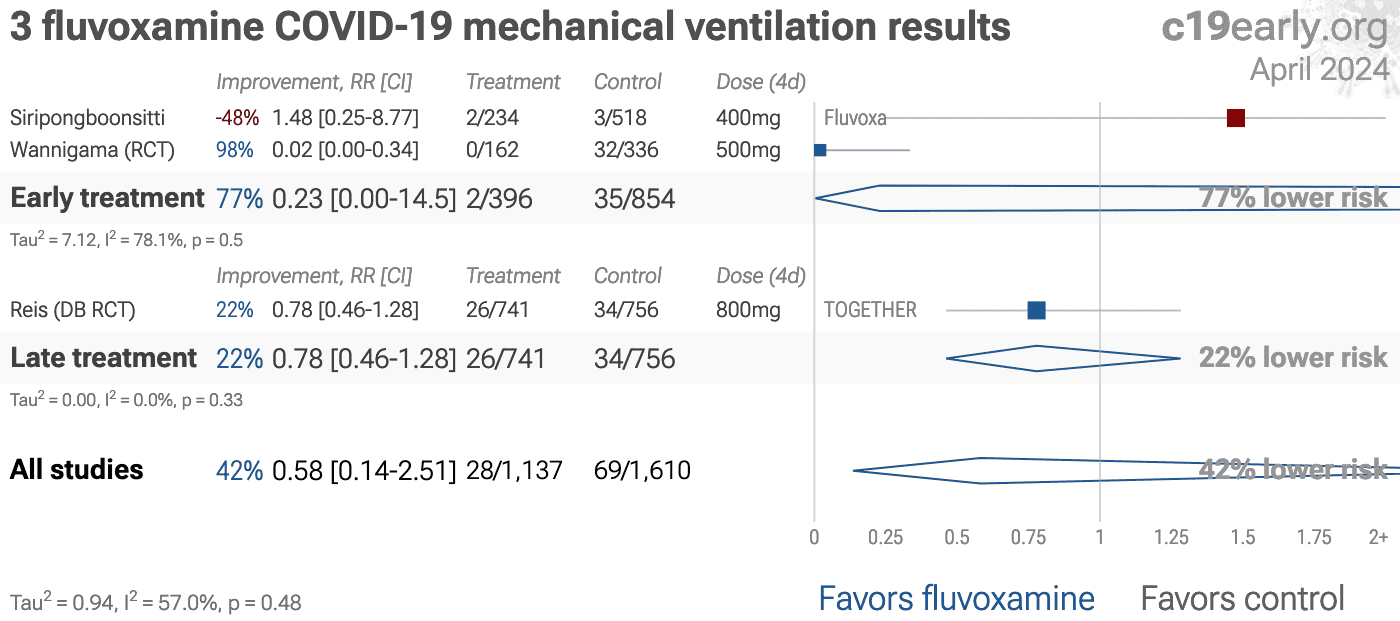
Figure 5. Random effects meta-analysis for ventilation.
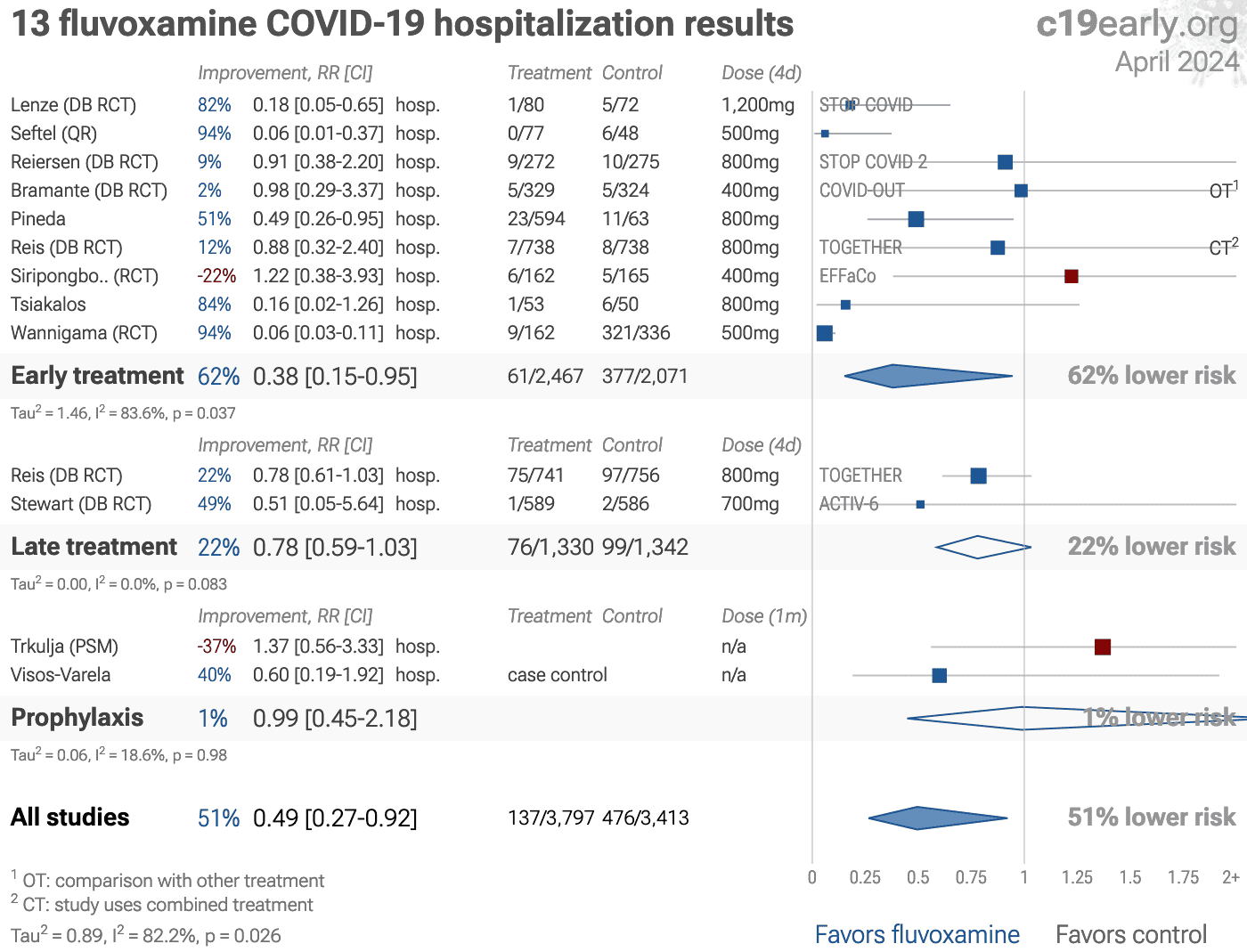
Figure 6. Random effects meta-analysis for hospitalization.
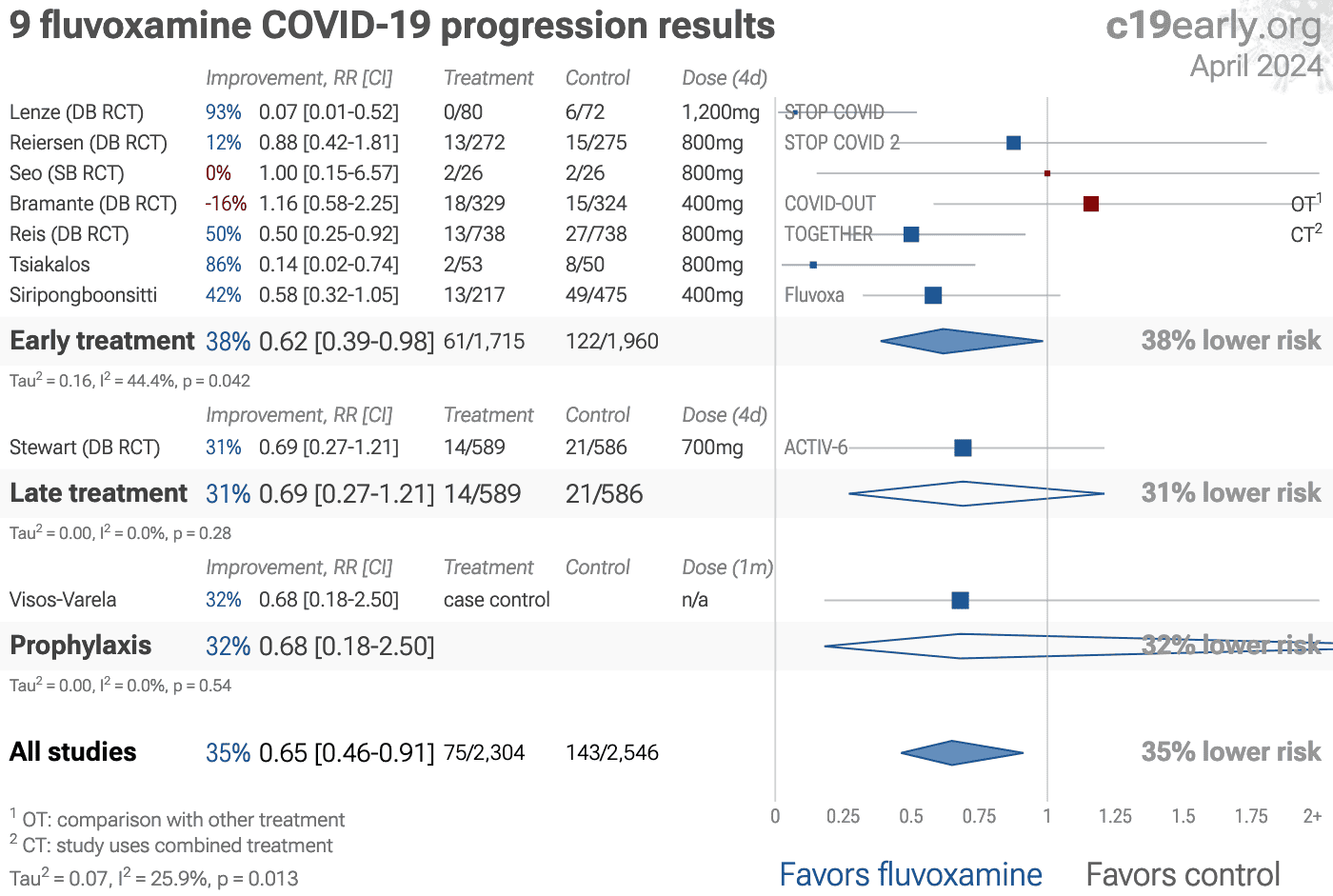
Figure 7. Random effects meta-analysis for progression.
Figure 8. Random effects meta-analysis for recovery.
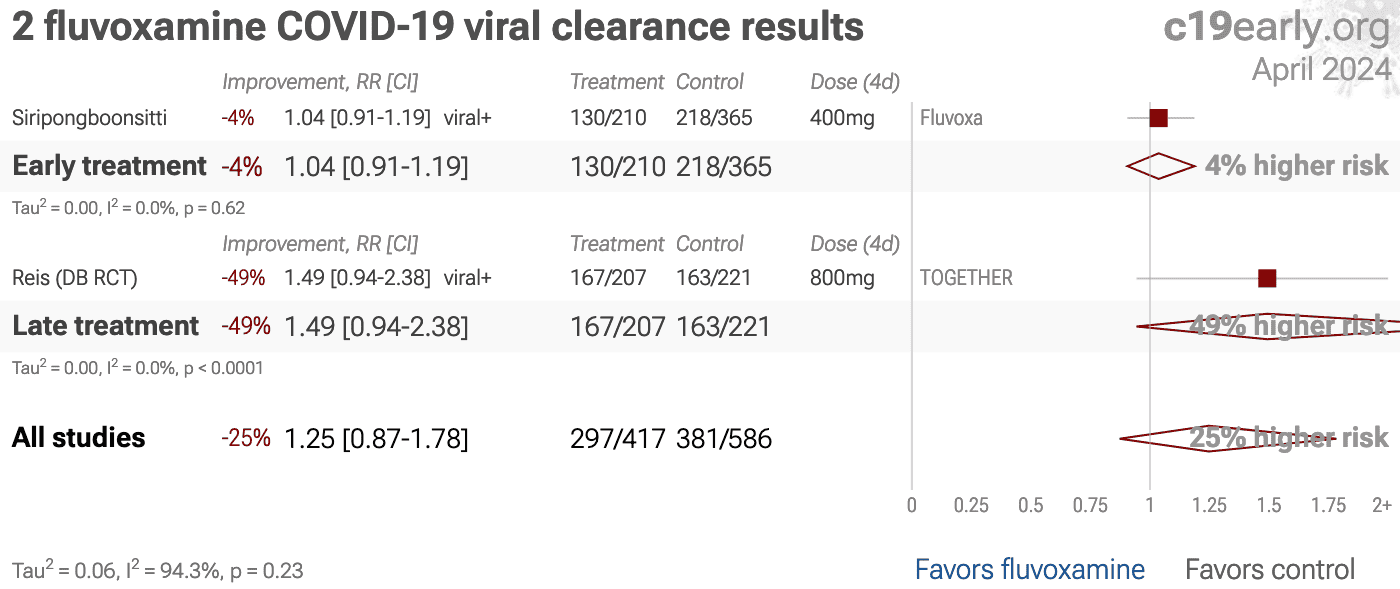
Figure 9. Random effects meta-analysis for viral clearance.
Figure 10. Random effects meta-analysis for peer reviewed studies.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Randomized Controlled Trials (RCTs)
Figure 11 and 12
show forest plots for a random effects meta-analysis of
all Randomized Controlled Trials and RCT mortality results.
Table 3 summarizes the results.
RCTs have a bias against finding an effect for interventions
that are widely available — patients that believe they need the
intervention are more likely to decline participation and take the
intervention. This is illustrated with the extreme example of an RCT showing
no significant differences for use of a parachute when jumping from a plane
[Yeh]. RCTs for fluvoxamine are more likely to enroll low-risk
participants that do not need treatment to recover, making the results less
applicable to clinical practice. This bias is likely to be greater for widely
known treatments.
Note that this bias does
not apply to the typical pharmaceutical trial of a new drug that is otherwise
unavailable.
Evidence shows that non-RCT trials can also provide reliable
results. [Concato] find that well-designed observational studies do
not systematically overestimate the magnitude of the effects of treatment
compared to RCTs. [Anglemyer] summarized reviews comparing RCTs to
observational studies and found little evidence for significant differences
in effect estimates.
[Lee] shows that only 14% of the guidelines
of the Infectious Diseases Society of America were based on RCTs. Evaluation
of studies relies on an understanding of the study and potential biases.
Limitations in an RCT can outweigh the benefits, for example excessive
dosages, excessive treatment delays, or Internet survey bias could have a
greater effect on results. Ethical issues may also prevent running RCTs for
known effective treatments. For more on issues with RCTs see [Deaton, Nichol].
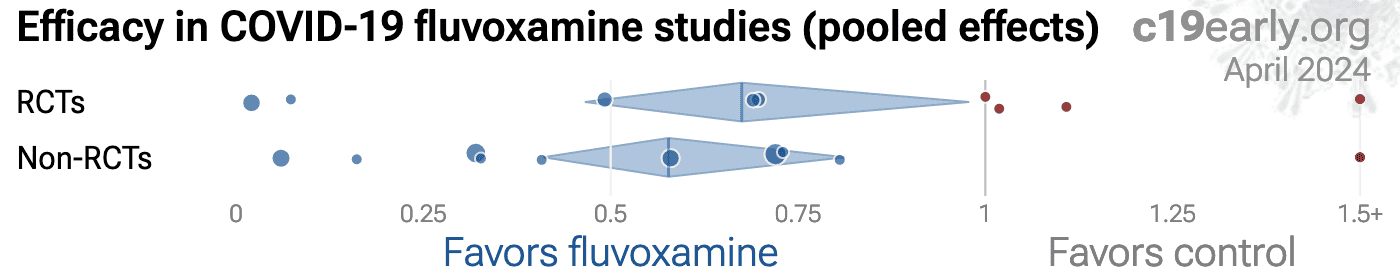
Figure 13. Randomized Controlled Trials. The
distribution of results for RCTs and other studies.
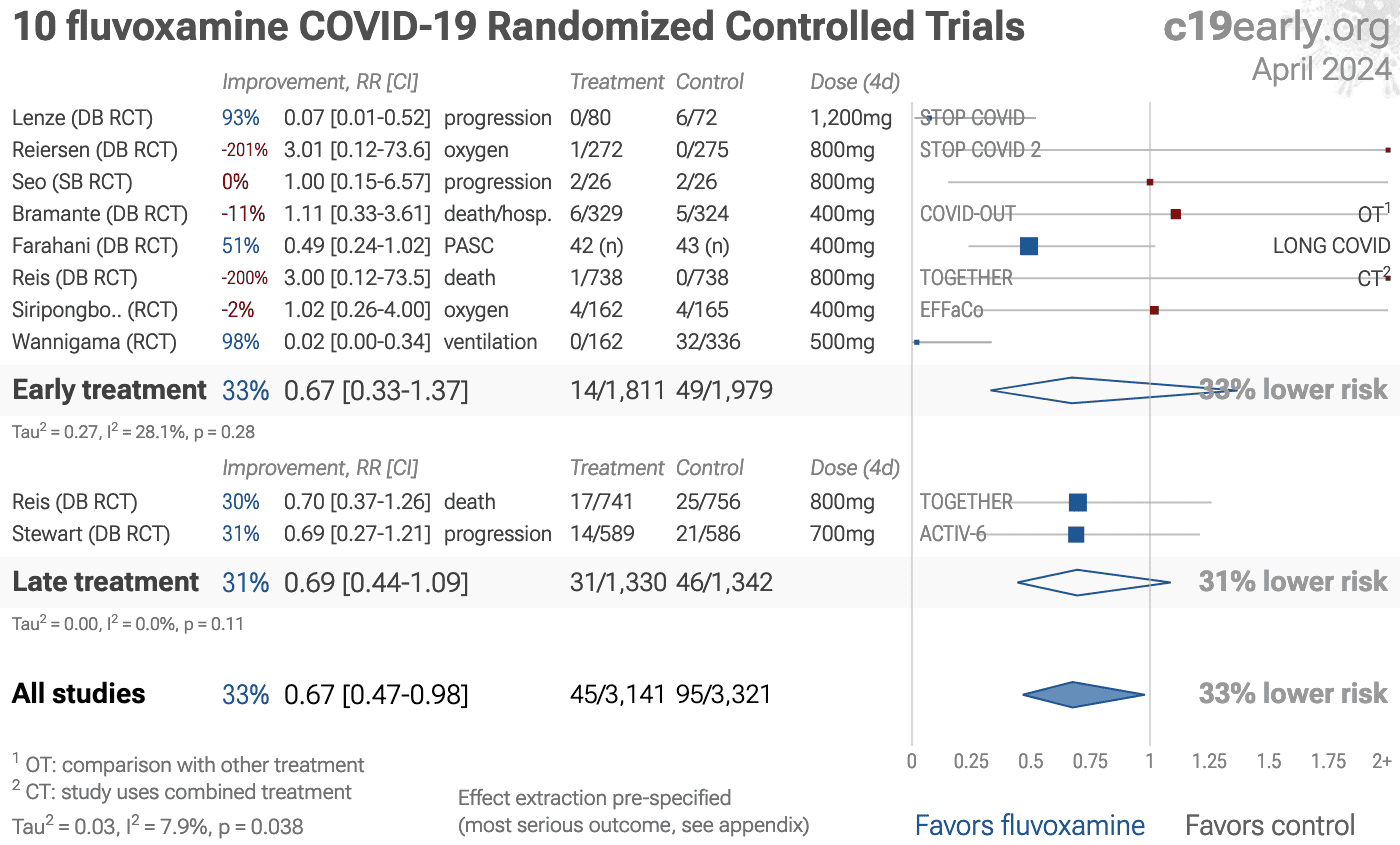
Figure 11. Random effects meta-analysis for all Randomized Controlled Trials.
This plot shows pooled effects, discussion can be found in the heterogeneity section,
and results for specific outcomes can be found in the individual outcome analyses.
Effect extraction is pre-specified, using the most serious outcome reported.
For details of effect extraction see the appendix.
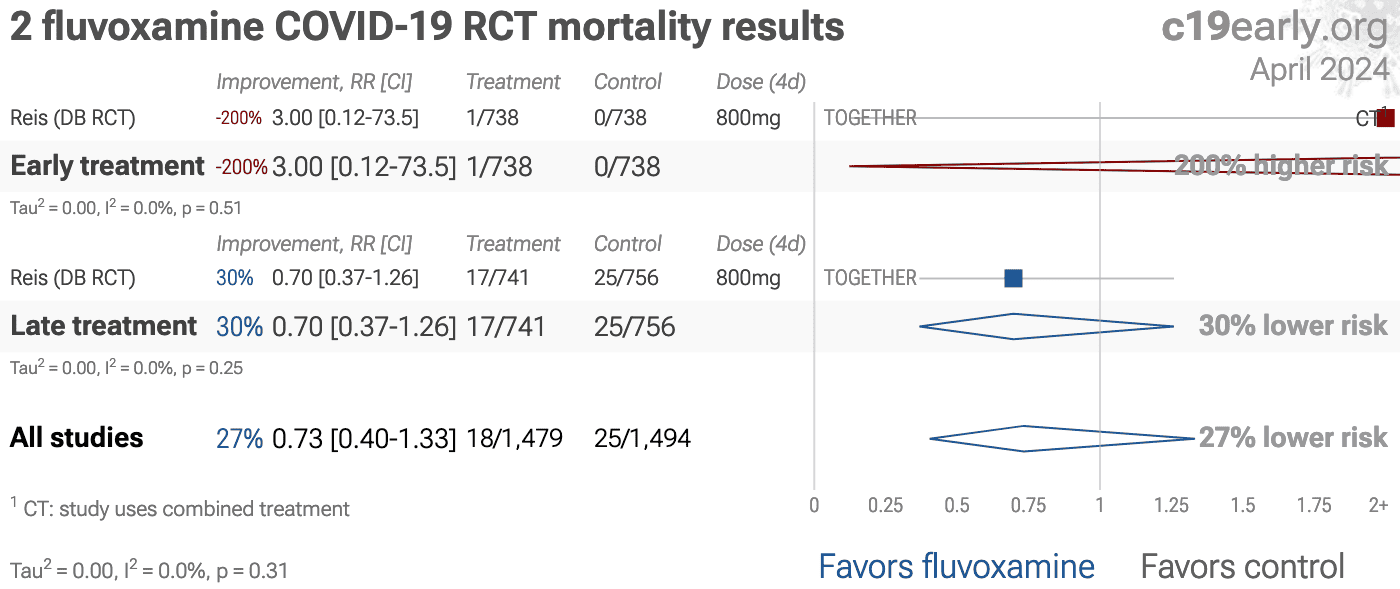
Figure 12. Random effects meta-analysis for RCT mortality results.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
| Treatment time | Number of studies reporting positive effects | Total number of studies | Percentage of studies reporting positive effects | Random effects meta-analysis results |
| Randomized Controlled Trials | 3 | 3 | 100% |
30% improvement RR 0.70 [0.37‑1.34] p = 0.28 |
| RCT mortality results | 1 | 1 | 100% |
30% improvement RR 0.70 [0.38‑1.28] p = 0.25 |
Table 3. Randomized Controlled Trial results.
Heterogeneity
Heterogeneity in COVID-19 studies arises from many factors including:
Treatment delay.
The time between infection
or the onset of symptoms and treatment may critically affect how well a
treatment works. For example an antiviral may be very effective when used
early but may not be effective in late stage disease, and may even be harmful.
Oseltamivir, for example, is generally only considered effective for influenza
when used within 0-36 or 0-48 hours [McLean, Treanor]. Other
medications might be beneficial for late stage complications, while early use
may not be effective or may even be harmful. Figure 14 shows
an example where efficacy declines as a function of treatment delay.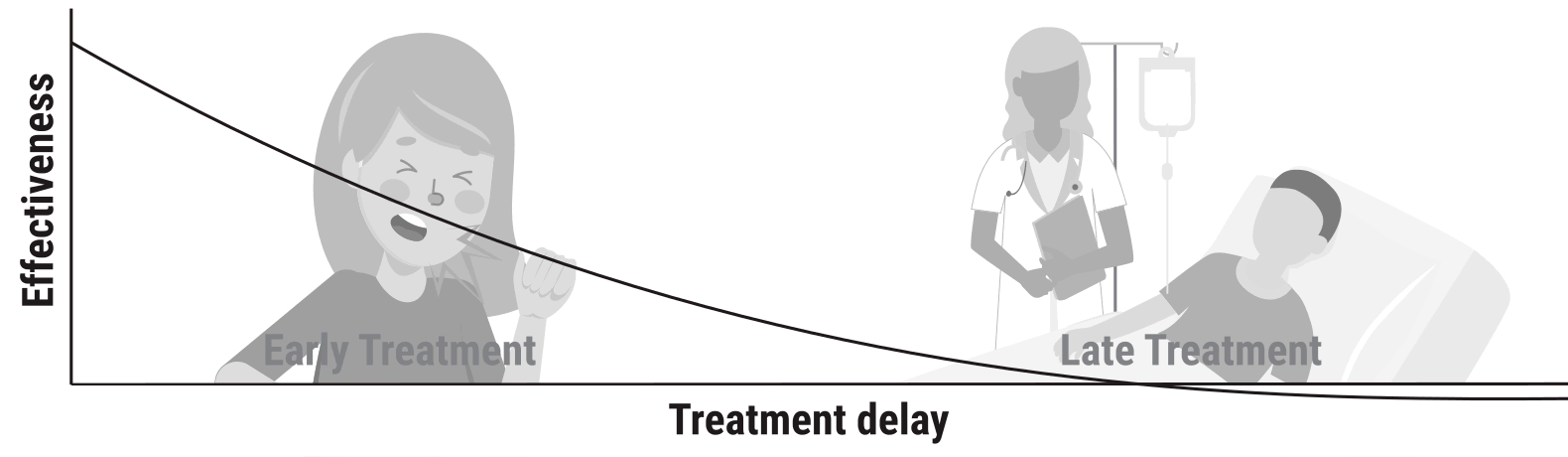
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 14. Effectiveness may depend critically
on treatment delay.
Patient demographics.
Details of the
patient population including age and comorbidities may critically affect how
well a treatment works. For example, many COVID-19 studies with relatively
young low-comorbidity patients show all patients recovering quickly with or
without treatment. In such cases, there is little room for an effective
treatment to improve results (as in [López-Medina]).Effect measured.
Efficacy may differ
significantly depending on the effect measured, for example a treatment may be
very effective at reducing mortality, but less effective at minimizing cases
or hospitalization. Or a treatment may have no effect on viral clearance while
still being effective at reducing mortality.Variants.
There are many different
variants of SARS-CoV-2 and efficacy may depend critically on the distribution
of variants encountered by the patients in a study. For example, the Gamma
variant shows significantly different characteristics
[Faria, Karita, Nonaka, Zavascki].Regimen.
Effectiveness may depend
strongly on the dosage and treatment regimen.Treatments.
The use of other
treatments may significantly affect outcomes, including anything from
supplements, other medications, or other kinds of treatment such as prone
positioning.The distribution of studies will alter the outcome of a meta
analysis. Consider a simplified example where everything is equal except for
the treatment delay, and effectiveness decreases to zero or below with
increasing delay. If there are many studies using very late treatment, the
outcome may be negative, even though the treatment may be very effective when
used earlier.
In general, by combining heterogeneous studies, as all meta
analyses do, we run the risk of obscuring an effect by including studies where
the treatment is less effective, not effective, or harmful.
When including studies where a treatment is less effective we
expect the estimated effect size to be lower than that for the optimal case.
We do not a priori expect that pooling all studies will create a
positive result for an effective treatment. Looking at all studies is valuable
for providing an overview of all research, important to avoid cherry-picking,
and informative when a positive result is found despite combining less-optimal
situations. However, the resulting estimate does not apply to specific cases
such as early treatment in high-risk populations.
Discussion
Publication bias.
Publishing is often biased
towards positive results, however evidence suggests that there may be a negative bias for
inexpensive treatments for COVID-19. Both negative and positive results are
very important for COVID-19, media in many countries prioritizes negative
results for inexpensive treatments (inverting the typical incentive for
scientists that value media recognition), and there are many reports of
difficulty publishing positive results
[Boulware, Meeus, Meneguesso].
For fluvoxamine, there is currently not
enough data to evaluate publication bias with high confidence.Conflicts of interest.
Pharmaceutical drug
trials often have conflicts of interest whereby sponsors or trial staff have a
financial interest in the outcome being positive. Fluvoxamine for COVID-19
lacks this because it is
off-patent, has multiple manufacturers, and is very low cost.
In contrast, most COVID-19 fluvoxamine trials have been run by
physicians on the front lines with the primary goal of finding the best
methods to save human lives and minimize the collateral damage caused by
COVID-19. While pharmaceutical companies are careful to run trials under
optimal conditions (for example, restricting patients to those most likely to
benefit, only including patients that can be treated soon after onset when
necessary, and ensuring accurate dosing), not all fluvoxamine trials
represent the optimal conditions for efficacy.Early/late vs. mild/moderate/severe.
Some analyses classify treatment based on early/late administration (as we do
here), while others distinguish between mild/moderate/severe cases. We note
that viral load does not indicate degree of symptoms — for example
patients may have a high viral load while being asymptomatic. With regard to
treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.Conclusion
Fluvoxamine is an effective treatment for COVID-19.
Meta analysis using the most serious outcome reported shows
34% [7‑53%] improvement. Results are similar for Randomized Controlled Trials and similar for peer-reviewed studies. Early treatment is more effective than late treatment.
Statistically significant improvements are seen for mortality and recovery. 4 studies from 4 independent teams in 3 different countries show statistically significant
improvements in isolation (1 for the most serious outcome).
Study Notes
[Calusic] Prospective PSM study of 51 COVID-19 ICU patients in Croatia and 51 matched controls, showing significantly lower mortality with treatment.
[Lenze] Presentation noting that STOP COVID 2 was terminated early for futility with only 30/551 cases of detioration and no significant treatment effect. The main results are not available yet, however partial results presented suggest that early treatment was more effective. NCT04668950. Hospitalization results are from https://www.medrxiv.org/content/10.1101/2021.12.17.21268008v1.
[Lenze (B)] RCT 152 outpatients, 80 treated with fluvoxamine showing lower progression with treatment (0 of 80 versus 6 of 72 control). STOP COVID trial. NCT04342663.
[Oskotsky] Retrospective database analysis of 83,584 patients in the USA, showing lower mortality with existing fluoxetine use in PSM analysis. There were 11 fluvoxamine patients, showing non-statistically significant higher mortality.
[Reis] Together Trial showing significantly lower hospitalization/extended ER visits with fluvoxamine treatment. Adherence was only 73.2%. Symptom onset was unspecified or >= 4 days for 57% of patients. The schedule of study activities specifies treatment administration only one day after randomization, adding an additional day delay. Overall mortality is high for the patient population. Results may be impacted by late treatment, poor SOC, and may be specific to local variants https://science.sciencemag.org/content/372/6544/815 https://www.thelancet.com/article/S0140-6736(21)00183-5/fulltext. Per-protocol analysis shows significantly improved results in this trial, however this may be subject to bias - the probability of adherence may be related to the probability of the outcome.
Regarding the combined hospitalization/extended ER observation outcome, authors have noted that at the study sites, extended medical observation was essentially equivalent to being hospitalized. “These were not standard emergency rooms but instead were COVID-19 emergency centers that were set up due to hospitals being overloaded,” Reiersen noted in an email to The Scientist. “A stay in these centers >6 hours was an indication that the patient was receiving care equivalent to hospitalization.”
Authors state "this study is only the second study to show an important treatment benefit for a repurposed drug in the early treatment population", however the actual number is at least 66 based on our database at the time of publication, using a conservative definition of at least 10% benefit (with statistical significance).
The total dose used is less than half of that in Lenze et al. There is an unusual amount of missing data - age is unknown for 6.5% of patients according to the sub-group analysis. Both age <=50 and >50 show better results on the primary outcome than the overall result. The number of placebo patients changed significantly between the preprint and journal version. The number of treatment patients with viral clearance results reduced significantly between the preprint and journal version. Also see https://twitter.com/Covid19Crusher/status/1430170252575395843. NCT04727424.
For other issues with this trial see: https://twitter.com/Covid19Crusher/status/1453726471499894787 https://twitter.com/Covid19Crusher/status/1453803654608269318.
[Seftel] Prospective quasi-randomized (patient choice) study with 125 outpatients, 77 treated with fluvoxamine, showing lower death/ICU admission (0 of 77 vs. 2 of 48), lower hospitalization (0 of 77 vs. 6 of 48), and faster recovery with treatment. Note that 12 treatment patients were added but are not reflected in the table in the paper (because the numbers had been previously published and the IRB did not allow updating the table).
We performed ongoing searches of PubMed, medRxiv,
ClinicalTrials.gov, The Cochrane Library, Google Scholar, Collabovid, Research
Square, ScienceDirect, Oxford University Press, the reference lists of other
studies and meta-analyses, and submissions to the site c19fluvoxamine.com. Search terms were fluvoxamine, filtered for papers containing the terms COVID-19, SARS-CoV-2, or coronavirus. Automated searches are performed
every few hours with notification of new matches.
All studies regarding the use of fluvoxamine for COVID-19 that report
a comparison with a control group are included in the main analysis.
We extracted effect sizes and associated data from all studies.
If studies report multiple kinds of effects then the most serious outcome is
used in pooled analysis, while other outcomes are included in the outcome
specific analyses. For example, if effects for mortality and cases are both
reported, the effect for mortality is used, this may be different to the
effect that a study focused on. If symptomatic results are reported at
multiple times, we used the latest time, for example if mortality results are
provided at 14 days and 28 days, the results at 28 days are used. Mortality
alone is preferred over combined outcomes.
Outcomes with zero events in both arms were not used (the next most serious
outcome is used — no studies were excluded). For example, in low-risk
populations with no mortality, a reduction in mortality with treatment is not
possible, however a reduction in hospitalization, for example, is still
valuable.
Clinical outcome is considered more important than PCR testing status. When
basically all patients recover in both treatment and control groups,
preference for viral clearance and recovery is given to results mid-recovery
where available (after most or all patients have recovered there is no room
for an effective treatment to do better).
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
When results provide an odds ratio, we computed the relative risk when
possible, or converted to a relative risk according to [Zhang].
Reported confidence intervals and p-values were used when available,
using adjusted values when provided. If multiple types of adjustments are
reported including propensity score matching (PSM), the PSM results are used.
When needed, conversion between reported p-values and confidence
intervals followed [Altman, Altman (B)], and Fisher's exact test was
used to calculate p-values for event data. If continuity correction for
zero values is required, we use the reciprocal of the opposite arm with the
sum of the correction factors equal to 1 [Sweeting].
Results are expressed with RR < 1.0 favoring treatment, and using the risk of
a negative outcome when applicable (for example, the risk of death rather than
the risk of survival). If studies only report relative continuous values such
as relative times, the ratio of the time for the treatment group versus the
time for the control group is used. Calculations are done in Python
(3.9.9) with
scipy (1.7.3), pythonmeta (1.26), numpy (1.21.4), statsmodels (0.14.0), and plotly (5.4.0).
Forest plots are computed using PythonMeta [Deng]
with the DerSimonian and Laird random effects model (the fixed effect
assumption is not plausible in this case) and inverse variance weighting.
We received no funding, this research is done in our spare
time. We have no affiliations with any pharmaceutical companies or political
parties.
We have classified studies as early treatment if most patients
are not already at a severe stage at the time of treatment, and treatment
started within 5 days of the onset of symptoms. If studies contain a mix of
early treatment and late treatment patients, we consider the treatment time of
patients contributing most to the events (for example, consider a study where
most patients are treated early but late treatment patients are included, and
all mortality events were observed with late treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only
considered effective when used within a shorter timeframe, for example 0-36 or
0-48 hours for oseltamivir, with longer delays not being effective
[McLean, Treanor].
A summary of study results is below. Please submit
updates and corrections at https://c19fluvoxamine.com/meta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| [Lenze], 8/20/2021, Double Blind Randomized Controlled Trial, USA, North America, preprint, 1 author. | risk of hospitalization, 7.3% lower, RR 0.93, p = 1.00, treatment 11 of 272 (4.0%), control 12 of 275 (4.4%), NNT 313. |
| [Lenze (B)], 11/12/2020, Double Blind Randomized Controlled Trial, USA, North America, peer-reviewed, 11 authors. | risk of progression, 92.7% lower, RR 0.07, p = 0.009, treatment 0 of 80 (0.0%), control 6 of 72 (8.3%), NNT 12, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), clinical deterioration over 15 days. |
| risk of hospitalization, 82.0% lower, RR 0.18, p = 0.009, treatment 1 of 80 (1.2%), control 5 of 72 (6.9%), NNT 18, COVID-19 hospitalization within 15 days, see supplemental appendix for details. | |
| [Seftel], 2/1/2021, prospective quasi-randomized (patient choice), USA, North America, peer-reviewed, 2 authors. | risk of death/ICU, 83.9% lower, RR 0.16, p = 0.15, treatment 0 of 77 (0.0%), control 2 of 48 (4.2%), NNT 24, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of hospitalization, 94.0% lower, RR 0.06, p = 0.003, treatment 0 of 77 (0.0%), control 6 of 48 (12.5%), NNT 8.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| risk of no recovery, 98.7% lower, RR 0.01, p < 0.001, treatment 0 of 77 (0.0%), control 29 of 48 (60.4%), NNT 1.7, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| [Calusic], 11/1/2021, prospective, propensity score matching, Croatia, Europe, peer-reviewed, 7 authors, 1 April, 2021 - 31 May, 2021. | risk of death, 42.0% lower, RR 0.58, p = 0.03, treatment 30 of 51 (58.8%), control 39 of 51 (76.5%), NNT 5.7, adjusted per study, propensity score matching. |
| [Reis], 8/23/2021, Double Blind Randomized Controlled Trial, Brazil, South America, peer-reviewed, 27 authors. | risk of death, 30.3% lower, RR 0.70, p = 0.24, treatment 17 of 741 (2.3%), control 25 of 756 (3.3%), NNT 99, odds ratio converted to relative risk, ITT. |
| risk of death, 90.8% lower, RR 0.09, p = 0.02, treatment 1 of 548 (0.2%), control 12 of 618 (1.9%), NNT 57, odds ratio converted to relative risk, per protocol. | |
| risk of mechanical ventilation, 22.2% lower, RR 0.78, p = 0.33, treatment 26 of 741 (3.5%), control 34 of 756 (4.5%), NNT 101, odds ratio converted to relative risk, ITT. | |
| risk of hospitalization, 21.6% lower, RR 0.78, p = 0.10, treatment 75 of 741 (10.1%), control 97 of 756 (12.8%), NNT 37, odds ratio converted to relative risk, ITT. | |
| extended ER observation or hospitalization, 32.0% lower, RR 0.68, p = 0.004, treatment 79 of 741 (10.7%), control 119 of 756 (15.7%), NNT 20, ITT. | |
| extended ER observation or hospitalization, 31.0% lower, RR 0.69, p = 0.006, treatment 78 of 740 (10.5%), control 115 of 752 (15.3%), NNT 21, mITT. | |
| extended ER observation or hospitalization, 66.0% lower, RR 0.34, p < 0.001, treatment 541, control 609, per protocol. | |
| risk of no virological cure, 49.3% higher, RR 1.49, p = 0.09, treatment 167 of 207 (80.7%), control 163 of 221 (73.8%), adjusted per study. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| [Oskotsky], 11/15/2021, retrospective, propensity score matching, USA, North America, peer-reviewed, 8 authors. | risk of death, 57.9% higher, RR 1.58, p = 0.62, treatment 2 of 11 (18.2%), control 19 of 165 (11.5%), fluvoxamine. |
| risk of death, 26.0% lower, RR 0.74, p = 0.04, treatment 48 of 481 (10.0%), control 956 of 7,215 (13.3%), NNT 31, fluoxetine. |
References
Almási et al., International Journal of Molecular Sciences, doi:10.3390/ijms21114046,
Lessons on the Sigma-1 Receptor in TNBS-Induced Rat Colitis: Modulation of the UCHL-1, IL-6 Pathway,
https://www.mdpi.com/1422-0067/21/11/4046/pdf.
Altman, D., BMJ, doi:10.1136/bmj.d2304,
How to obtain the P value from a confidence interval,
https://www.bmj.com/content/343/bmj.d2304.
Altman (B) et al., BMJ, doi:10.1136/bmj.d2090,
How to obtain the confidence interval from a P value,
https://www.bmj.com/content/343/bmj.d2090.
Anderson, G., Psychopharmacology, doi:10.1007/s00213-020-05753-z,
Fluvoxamine, melatonin and COVID-19,
http://link.springer.com/article/1..7/s00213-020-05753-z/fulltext.html.
Anglemyer et al., Cochrane Database of Systematic Reviews 2014, Issue 4, doi:10.1002/14651858.MR000034.pub2,
Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials,
https://www.cochranelibrary.com/cd..0.1002/14651858.MR000034.pub2/full.
Battinelli, E., Blood, doi:10.1182/blood.2020007805,
COVID-19 concerns aggregate around platelets,
http://dx.doi.org/10.1182/blood.2020007805.
Boulware, D.,
Comments regarding paper rejection,
https://twitter.com/boulware_dr/status/1311331372884205570.
Calusic et al., British Journal of Clinical Pharmacology, doi:10.1111/bcp.15126,
Safety and efficacy of fluvoxamine in COVID-19 ICU patients: an open label, prospective cohort trial with matched controls,
https://bpspubs.onlinelibrary.wiley.com/doi/10.1111/bcp.15126.
Camp et al., Journal of Inorganic Biochemistry, doi:10.1016/j.jinorgbio.2021.111546,
Melatonin interferes with COVID-19 at several distinct ROS-related steps,
http://dx.doi.org/10.1016/j.jinorgbio.2021.111546.
Carpinteiro et al., Journal of Biological Chemistry, doi:10.1016/j.jbc.2021.100701,
Inhibition of acid sphingomyelinase by ambroxol prevents SARS-CoV-2 entry into epithelial cells,
http://dx.doi.org/10.1016/j.jbc.2021.100701.
Carpinteiro (B) et al., Cell Reports Medicine, doi:10.1016/j.xcrm.2020.100142,
Pharmacological Inhibition of Acid Sphingomyelinase Prevents Uptake of SARS-CoV-2 by Epithelial Cells,
http://dx.doi.org/10.1016/j.xcrm.2020.100142.
Concato et al., NEJM, 342:1887-1892, doi:10.1056/NEJM200006223422507,
https://www.nejm.org/doi/full/10.1056/nejm200006223422507.
Deaton et al., Social Science & Medicine, 210, doi:10.1016/j.socscimed.2017.12.005,
Understanding and misunderstanding randomized controlled trials,
https://www.sciencedirect.com/science/article/pii/S0277953617307359.
Faria et al., Science, doi:10.1126/science.abh2644,
Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil,
https://www.science.org/lookup/doi/10.1126/science.abh2644.
Hashimoto et al., European Archives of Psychiatry and Clinical Neuroscience, doi:10.1007/s00406-021-01326-z,
Old drug fluvoxamine, new hope for COVID-19
,
https://link.springer.com/article/10.1007/s00406-021-01326-z.
Hoertel et al., Molecular Psychiatry, doi:10.1038/s41380-021-01254-3,
Repurposing antidepressants inhibiting the sphingomyelinase acid/ceramide system against COVID-19: current evidence and potential mechanisms,
https://www.nature.com/articles/s41380-021-01254-3.
Hooper, P., Cell Stress and Chaperones, doi:10.1007/s12192-020-01126-9,
COVID-19 and heme oxygenase: novel insight into the disease and potential therapies,
https://link.springer.com/article/10.1007%2Fs12192-020-01126-9.
Hooper (B), P., Cell Stress and Chaperones, doi:10.1007/s12192-021-01246-w,
Heme oxygenase agonists—fluvoxamine, melatonin—are efficacious therapy for Covid-19,
https://link.springer.com/article/..7/s12192-021-01246-w/fulltext.html.
Karita et al., medRxiv, doi:10.1101/2021.08.27.21262754,
Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection,
https://www.medrxiv.org/content/10.1101/2021.08.27.21262754v1.
Lee et al., Arch Intern Med., 2011, 171:1, 18-22, doi:10.1001/archinternmed.2010.482,
Analysis of Overall Level of Evidence Behind Infectious Diseases Society of America Practice Guidelines,
https://jamanetwork.com/journals/j..nternalmedicine/fullarticle/226373.
Lenze, E.,
Fluvoxamine for Early Treatment of COVID-19: The STOP COVID Clinical Trials,
https://dcricollab.dcri.duke.edu/sites/NIHKR/KR/GR-Slides-08-20-21.pdf.
Lenze (B) et al., JAMA, doi:10.1001/jama.2020.22760,
Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial,
https://jamanetwork.com/journals/jama/fullarticle/2773108.
López-Medina et al., JAMA, doi:10.1001/jama.2021.3071,
Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial,
https://jamanetwork.com/journals/jama/fullarticle/2777389.
McLean et al., Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100,
Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4525010/.
Meneguesso, A.,
Médica defende tratamento precoce da Covid-19,
https://www.youtube.com/watch?v=X5FCrIm_19U.
Nichol et al., Injury, 2010, doi: 10.1016/j.injury.2010.03.033,
Challenging issues in randomised controlled trials,
https://www.injuryjournal.com/article/S0020-1383(10)00233-0/fulltext.
Nonaka et al., International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003,
SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021,
https://www.sciencedirect.com/science/article/pii/S1201971221006354.
Norinder et al., Biomedicine & Pharmacotherapy, doi:10.1016/j.biopha.2020.110582,
Existing highly accumulating lysosomotropic drugs with potential for repurposing to target COVID-19,
http://dx.doi.org/10.1016/j.biopha.2020.110582.
Oskotsky et al., JAMA Network Open, doi:10.1001/jamanetworkopen.2021.33090,
Mortality Risk Among Patients With COVID-19 Prescribed Selective Serotonin Reuptake Inhibitor Antidepressants,
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2786136.
Pfizer,
Pfizer Second Quarter 2021 Earnings Teleconference,
https://s21.q4cdn.com/317678438/fi../Q2-2021-Earnings-Charts-FINAL.pdf.
Ramos et al., Antioxidants, doi:10.3390/antiox10071152 ,
The Coronavirus Disease 2019 (COVID-19): Key Emphasis on Melatonin Safety and Therapeutic Efficacy,
https://www.mdpi.com/2076-3921/10/7/1152/htm.
Reis et al., The Lancet Global Health, doi:10.1016/S2214-109X(21)00448-4 (preprint 8/23/2021),
Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial,
https://www.thelancet.com/journals../PIIS2214-109X(21)00448-4/fulltext.
Seftel et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofab050,
Prospective cohort of fluvoxamine for early treatment of COVID-19,
https://academic.oup.com/ofid/adva..e/doi/10.1093/ofid/ofab050/6124100.
Sukhatme et al., Front. Pharmacol., doi:10.3389/fphar.2021.652688,
Fluvoxamine: A Review of Its Mechanism of Action and Its Role in COVID-19,
https://www.frontiersin.org/articles/10.3389/fphar.2021.652688/full.
Sweeting et al., Statistics in Medicine, doi:10.1002/sim.1761,
What to add to nothing? Use and avoidance of continuity corrections in meta‐analysis of sparse data,
https://onlinelibrary.wiley.com/doi/10.1002/sim.1761.
Treanor et al., JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016,
Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial,
https://jamanetwork.com/journals/jama/fullarticle/192425.
Yeh et al., BMJ, doi:10.1136/bmj.k5094 ,
Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial,
https://www.bmj.com/content/363/bmj.k5094.
Zavascki et al., Research Square, doi:10.21203/rs.3.rs-910467/v1,
Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil,
https://www.researchsquare.com/article/rs-910467/v1.
Zhang et al., JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690,
What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes,
https://jamanetwork.com/journals/jama/fullarticle/188182.
Please send us corrections, updates, or comments. Vaccines and treatments are both extremely valuable and complementary. All
practical, effective, and safe means should be used. Elimination of COVID-19
is a race against viral evolution. No treatment, vaccine, or intervention is
100% available and effective for all current and future variants. Denying the
efficacy of any method increases the risk of COVID-19 becoming endemic; and
increases mortality, morbidity, and collateral damage. We do not provide
medical advice. Before taking any medication, consult a qualified physician
who can provide personalized advice and details of risks and benefits based
on your medical history and situation. Treatment protocols for physicians are
available from the FLCCC.