8/23 Late treatment study
et al., The Lancet Global Health, doi:10.1016/S2214-109X(21)00448-4 (preprint 8/23/2021) (Peer Reviewed)
Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial
Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial
Together Trial showing significantly lower hospitalization/extended ER visits with fluvoxamine treatment. Adherence was only 73.2%. Symptom onset was unspecified or >= 4 days for 57% of patients. The schedule of study activities specifies treatment administration only one day after randomization, adding an additional day delay. Overall mortality is high for the patient population. Results may be impacted by late treatment, poor SOC, and may be specific to local variants [1, 2]. Per-protocol analysis shows significantly improved results in this trial. Authors note that ITT analysis provides more real-world evidence, however RCTs do not provide real-world evidence. For a drug like fluvoxamine, which is widely available, and a condition like COVID-19, which has a significant risk of death and must be treated immediately for best results, RCTs are biased toward participants that do not need help to recover, or do not believe that the drug will help. (Because patients can decline participation and take the drug). Notably, the remaining patients that choose to participate are less likely to believe adherence is important. In real-world use, including patients that decline RCT participation, and with patients informed of the benefit, adherence is likely to be much better. Note that per-protocol analysis could affect randomization.The primary outcome changed in the March 21 clinicaltrials.gov update (observation >12hrs changed to >6hrs). This is not explained or mentioned in the paper.Authors state "this study is only the second study to show an important treatment benefit for a repurposed drug in the early treatment population", however the actual number is at least 66 based on our database at the time of publication, using a conservative definition of at least 10% benefit (with statistical significance).The total dose used is less than half of that in Lenze et al. There is an unusual amount of missing data - age is unknown for 6.5% of patients according to the sub-group analysis. Both age <=50 and >50 show better results on the primary outcome than the overall result. The number of placebo patients changed significantly between the preprint and journal version. The number of treatment patients with viral clearance results reduced significantly between the preprint and journal version. Also see [3]. NCT04727424.For other issues with this trial see: [4, 5].
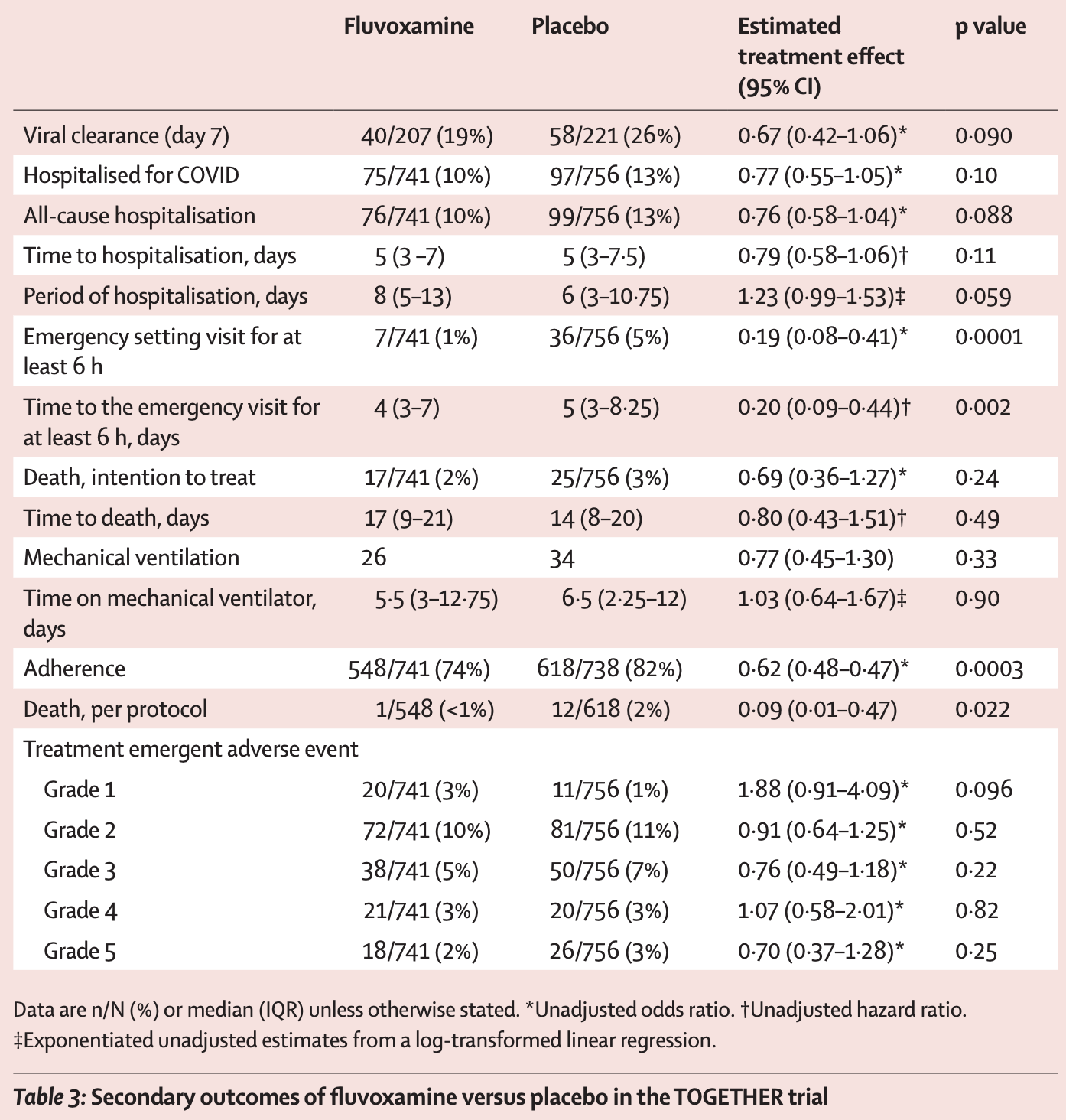
risk of death, 30.3% lower, RR 0.70, p = 0.24, treatment 17 of 741 (2.3%), control 25 of 756 (3.3%), odds ratio converted to relative risk, ITT.
risk of death, 90.8% lower, RR 0.09, p = 0.02, treatment 1 of 548 (0.2%), control 12 of 618 (1.9%), odds ratio converted to relative risk, per protocol.
risk of mechanical ventilation, 22.2% lower, RR 0.78, p = 0.33, treatment 26 of 741 (3.5%), control 34 of 756 (4.5%), odds ratio converted to relative risk, ITT.
risk of hospitalization, 21.6% lower, RR 0.78, p = 0.10, treatment 75 of 741 (10.1%), control 97 of 756 (12.8%), odds ratio converted to relative risk, ITT.
extended ER observation or hospitalization, 66.0% lower, RR 0.34, p < 0.001, treatment 541, control 609, per protocol.
extended ER observation or hospitalization, 32.0% lower, RR 0.68, p = 0.004, treatment 79 of 741 (10.7%), control 119 of 756 (15.7%), ITT.
extended ER observation or hospitalization, 31.0% lower, RR 0.69, p = 0.006, treatment 78 of 740 (10.5%), control 115 of 752 (15.3%), mITT.
risk of no virological cure, 49.3% higher, RR 1.49, p = 0.09, treatment 167 of 207 (80.7%), control 163 of 221 (73.8%), adjusted per study.
Reis et al., 8/23/2021, Double Blind Randomized Controlled Trial, Brazil, South America, peer-reviewed, 27 authors.
Effect extraction follows pre-specified rules
prioritizing more serious outcomes. For an individual study the most serious
outcome may have a smaller number of events and lower statistical signficance,
however this provides the strongest evidence for the most serious outcomes
when combining the results of many trials.
[1] science.sciencemag.org/content/372/6544/815
[2] thelancet.com/article/S0140-6736(21)00183-5/fulltext
[3] twitter.com/Covid19Crusher/status/1430170252575395843
[4] twitter.com/Covid19Crusher/status/1453726471499894787
[5] twitter.com/Covid19Crusher/status/1453803654608269318
Please send us corrections, updates, or comments. Vaccines and treatments are both extremely valuable and complementary. All
practical, effective, and safe means should be used. Elimination of COVID-19
is a race against viral evolution. No treatment, vaccine, or intervention is
100% available and effective for all current and future variants. Denying the
efficacy of any method increases the risk of COVID-19 becoming endemic; and
increases mortality, morbidity, and collateral damage. We do not provide
medical advice. Before taking any medication, consult a qualified physician
who can provide personalized advice and details of risks and benefits based
on your medical history and situation. Treatment protocols for physicians are
available from the FLCCC.