9/2 Review
et al., European Archives of Psychiatry and Clinical Neuroscience, doi:10.1007/s00406-021-01326-z (Review) (Peer Reviewed)
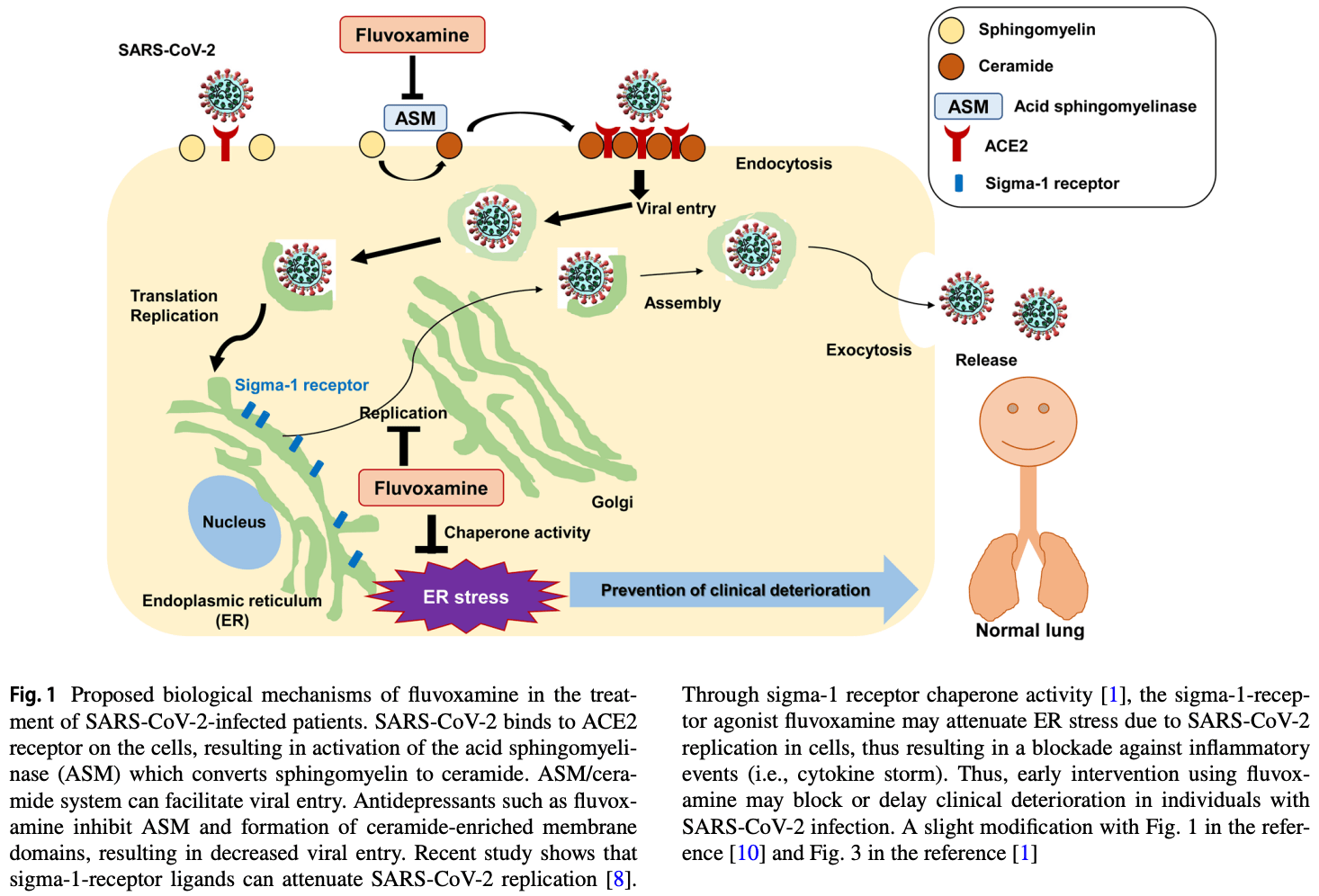
Old drug fluvoxamine, new hope for COVID-19
Old drug fluvoxamine, new hope for COVID-19
Review of research supporting the use of fluvoxamine for COVID-19. Authors note the favorable safety profiles, widespread availability, very low cost, and oral administration.
Hashimoto et al., 9/2/2021, peer-reviewed, 3 authors.
Please send us corrections, updates, or comments. Vaccines and treatments are both extremely valuable and complementary. All
practical, effective, and safe means should be used. Elimination of COVID-19
is a race against viral evolution. No treatment, vaccine, or intervention is
100% available and effective for all current and future variants. Denying the
efficacy of any method increases the risk of COVID-19 becoming endemic; and
increases mortality, morbidity, and collateral damage. We do not provide
medical advice. Before taking any medication, consult a qualified physician
who can provide personalized advice and details of risks and benefits based
on your medical history and situation. Treatment protocols for physicians are
available from the FLCCC.